Ella King*
This policy report will identify and address the financial, geographical and social obstacles same-sex female couples in the UK face when accessing in vitro fertilisation (IVF). It also proposes practical yet achievable, long and short-term actions that the government can take to ensure same-sex couples have equitable access to IVF.
Overview of the key findings and proposed recommendations.
Accessing IVF as a same-sex female couple is comparable to scaling a wall with a damaged ladder. The financial, geographical, and social obstacles faced by same-sex female partners are holding them back – making the climb tougher due to the broken equipment. Many members of the LGBTQ+ community subsequently find themselves stuck. Therefore, a reconstruction of the ‘ladder’ is needed to ensure a safer and fairer climb, enabling everyone to reach the top and access IVF. This reconstruction can be achieved by reforming policies to level the playing field for same-sex female couples to access IVF. This will ensure that no one is held back by damaged systems.
This report identifies the key issues and explains them using data, statistics and real-life stories before suggesting some realistic recommendations. The injustices of the additional barriers same-sex female couples are forced to endure in the pursuit of creating a family, and the steps that must be taken to improve this are set out.
This research will be looking at the barriers to IVF – one of the techniques available to assist people suffering from fertility issues. In the process of IVF, an egg is taken from a woman's ovaries and fertilised outside of the body, in a lab, with donor sperm.(1) Once fertilised, the egg is then placed into either woman’s womb as an embryo. In some cases, a donated egg may be used.
It is important to note that IVF is different from intrauterine insemination (IUI). IUI is a form of artificial insemination (AI) that helps a woman get pregnant by inserting the sperm directly into the uterus during ovulation.(2) The key difference is that IVF takes place outside the body, and IUI takes place inside. For the purposes of this research, the issues in accessibility refer to those of IVF specifically; however, one must not underestimate the challenges in accessing IUI.
The first documented UK IVF birth was on the 25th of July, 1978 when Louise Joy Brown was born at Oldham General Hospital(3) with the assistance of Drs. Patrick Steptoe and Robert Edwards.(4) Despite the initial “religious, ethical, and legal”(5) concerns, IVF has been an increasingly accessed form of fertility treatment for those suffering from fertility issues in society today.(6) The process is still relatively similar to that which Mrs. Brown underwent, namely, “[d]uring a natural cycle, an egg was harvested, fertilized in vitro in a petri dish, and, two days later, a single embryo was transferred into her uterus and resulted in the birth nine months later”.(7)
This monumental scientific breakthrough was accomplished with a heterosexual couple, yet same-sex couples did not enjoy the same access. This was because discrimination and homophobia were rife in the healthcare profession in the late 20th century – as evidenced by the increased use of aversion therapy at the international level in the 1950s.(8) Nevertheless, in modern society, the Equality Act 2010 and the Human Fertilisation and Embryology Act 2008 both help to ensure that same-sex couples have equal access to fertility treatment by criminalising discrimination based on sexual orientation, and broadening the welfare clause and legal parenthood provisions to better countenance female same-sex couple parenthood.(9) This has been a progressive step in ensuring equal access to IVF. Furthermore, the recent scrapping of mandatory screening for same-sex female couples (only) who wanted to conceive using IVF(10) continues to show this more level playing field between heterosexual and homosexual couples.
Despite this, significant challenges remain, with 36% of same-sex couples who had children claiming they faced barriers when starting their families, the most common being the financial challenge imposed by the high costs of treatment.(11) These legislative changes have clearly not done enough for same-sex female couples who rightfully deserve fair access to IVF. The next segment will detail three key areas where further changes are needed to ensure equitable accessibility.
A major barrier for same-sex female couples in accessing IVF is the extortionate cost that is incurred in trying to receive treatment from the National Health Service (NHS). A single round of IVF in the UK is around £5,000 if privately funded.(12) For many people this is simply not possible to do. Therefore, in a bid to increase accessibility of IVF for all, the NHS provides a service in which they will fund the treatment if certain conditions are met. It is here, in the ‘criteria’, that the problem lies, as same-sex couples are required to self-fund multiple rounds of artificial insemination before being granted NHS funding for IVF(13) – a financial hurdle that heterosexual couples do not face.
The criteria are set by Integrated Care Boards (which replaced the Clinical Commissioning Groups in 2022)(14) which are independent, statutory NHS bodies throughout England. In Canterbury, the Kent and Medway ICB governs the criteria one must meet to receive NHS-funded IVF treatment. Although most of the criteria are applicable for all, such as the requirements to be under 40 and a non-smoker,(15), the requirement to prove subfertility (fertility problems) creates an unfair disadvantage for same-sex female couples.(16) It states that patients must “have not conceived after 2 years of regular unprotected sexual intercourse”(17) or, for same-sex couples, “patients have undergone 12 unsuccessful cycles of artificial insemination, where 6 or more are by intrauterine insemination”.(18) Although up to 6 cycles of NHS-funded IUI may be available to eligible patients, this is not certain – as the term ‘may’ suggests. The individual must meet a strict set of conditions, such as being under 40 and having no previous children.(19) Thus, the requirement essentially forces same-sex couples to self-fund cycles of IUI and/or AI, whereas heterosexual couples only have to prove they have tried to conceive via sexual intercourse for 2 years – a free alternative. Same-sex female couples, therefore, may need to spend considerably more money just to try and get funding for IVF, defeating the whole purpose of why people apply for it in the first place. This can cause a significant financial burden on many same-sex couples, which is exacerbated by the state of the UK’s current financial affairs. A recent study has shown that 44% of UK adults now live in financially vulnerable circumstances.(20) As such, for many same-sex couples the ability to fund such expensive treatment is practically impossible due to financial hardships.
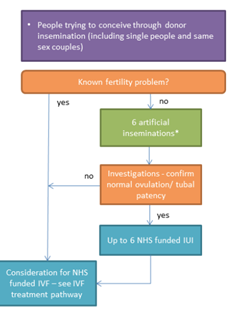
Diagram of the process of proving sub-fertility from Kent and Medway ICB, Schedule of policy statements for assisted reproductive technologies (ART) for Kent and Medway Integrated Care Board (24 June 2024), p.17.
This unfair barrier to funding was highlighted when a lesbian couple from Windsor – Megan Bacon-Evans and her wife Whitney – accused Frimley CCG of financially penalising them due to their sexuality. They stated that they had to pay “tens of thousands of pounds to become eligible for NHS-funded IVF”.(21) This issue creates such an unfair barrier for LGBTQ+ individuals who cannot prove infertility by sexual intercourse for 2 years. As a result, female same-sex couples achieve one of the lowest levels of NHS funding because they cannot reach this disproportionate criterion.(22)
It is imperative that the government takes action to reassess this criterion that unfairly hinders same-sex female couples from accessing NHS-funded IVF. An immediate change must be made to the criteria of ICBs to ensure access to IVF funding is on equal terms between heterosexual couples and same-sex couples. The government should remove the requirement for same-sex couples to undergo more than 6 rounds of self-funded artificial insemination before IVF treatment and reduce this number so that those who do need to prove subfertility by AI are not having to fund it themselves. This will create a more level playing field and reduce the financial barrier to NHS-funded IVF.
Additionally, a longer-term solution that can be implemented is a payment plan system, similar to a Lifetime ISA, for those who are considering IVF privately. Like an ISA, contributions by the individuals will be matched by government funds to allow more people to access IVF without needing the NHS to fund it. This will take the burden off NHS-funded treatments as more people will be able to pay to go privately, whilst simultaneously not overburdening the economy.
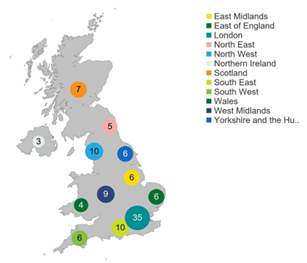
Number of clinics licensed to provide fertility treatment by geographical area, 2022/23. Diagram from Human Fertilisation and Embryology Authority,‘State of the Fertility Sector 2022/23’ (HFEA, 12 Sept 2023), section 3.
The geographical accessibility of IVF clinics is another barrier due to the lack of equipped clinics in more rural areas, and the varying requirements for NHS funding creating a ‘postcode lottery’. As the image here suggests, there is a clear lack of fertility clinics in rural areas. In 2022/23, 107 clinics were licensed by the HFEA to provide fertility treatment, the largest number being based in London.(23) However, of these approved clinics, only 61 catered to NHS-funded IVF treatment. This geographical disparity of clinics, along with the limited NHS option, reduces accessibility to IVF. In turn, many must travel far or seek expensive private treatment closer to home. This further exacerbates the inequalities in reproductive healthcare, as IVF is a key form of treatment for same-sex female couples due to their unique needs, yet many clinics are not equipped to provide it. In turn, this disproportionately affects same-sex female couples compared to heterosexual couples.
There are also accessibility issues amongst clinics themselves, creating a ‘postcode lottery’. This relates to ICBs across England having different eligibility criteria that individuals must meet to be given NHS funding. As noted previously, one of the Kent and Medway ICB criteria for NHS-funded IVF is proving subfertility by having undergone 12 unsuccessful cycles of AI, with 6 or more by IUI.(24) This is problematic as undergoing 12 cycles of AI is not the standard everywhere. Three quarters of ICBs (76%) require a minimum of three cycles of AI for patients to prove their “fertility status”, whereas 29 ICBs (27%) require between 10 and 12 cycles of AI.(25)
This shocking disparity can be best seen through the story of Emma and Helen. These two women from outside of Bristol were required, by the NHS Bristol, North Somerset and South Gloucestershire ICB, to pay for 6 cycles of AI before qualifying for a single round of NHS-funded IVF. However, just 30 miles down the road at Somerset NHS Trust ICB, they would have 9 cycles of AI and a round of IVF both funded by the NHS.(26) This is a display of the postcode lottery in action, as depending on where you live, you either strike ‘lucky’ and receive complete NHS funding, or you must self-fund multiple rounds of AI just to meet the criteria of NHS-funded IVF. For many like Emma and Helen, they “can’t afford to keep trying”.(27) This inconsistency in the eligibility criteria for NHS funding across ICBs in the UK creates an unfair barrier to accessing IVF. It forces many, like Emma and Helen, to undergo expensive AI cycles to meet these thresholds that often differ if one was from the next town. It ultimately makes NHS-funded IVF treatments inequitable and dependent on one's geographical location.
The government has tried, and failed, to address this issue. In 2022, the Women’s Health Strategy for England report recognised the need to combat the postcode lottery issue,(28) pledging to relieve additional barriers to IVF for same-sex couples and specifying that there should be “no requirement for self-funding and the NHS treatment pathway for female same-sex couples will start with 6 cycles of artificial insemination”.(29) However, many ICBs have not implemented the necessary reforms, and still requiring “female same-sex couples to self-fund at least six cycles of IUI”(30) to prove subfertility for NHS funding. As of April 2024, only 4 of the 42 ICBs in England have made changes.(31)
A long-term resolution that needs to be implemented is nationwide standards for clinic criteria on NHS funding. This would ensure that all clinics are adhering to the same criteria, subsequently getting rid of this postcode lottery. Such a recommendation was previously made in 2022; however, it has been rather unsuccessful due to the lack of enforcement initiative. As a result, the nationwide standards should be implemented within a specific time frame, or ICBs will be penalised with cost sanctions or legal action. This will ensure conformity.
An immediate way to address the disparity in geographical accessibility of IVF is to utilise technological advancements to reduce the need to travel to clinics unless necessary. Offering consultations online via Zoom or phone calls will be a good way to combat the lack of access to clinics in more rural areas, as it would not require individuals to travel far and often – only when needed for removing eggs and placing the fertilised egg back into the uterus. Although this does not completely solve the long-standing issue of the lack of facilities, it is a step in opening up access to IVF.
The stigma around same-sex couples in our heteronormative society has implications for accessing IVF treatments due to fear of discrimination created by society. The opinion of society heavily influences the effectiveness of any legislative/policy change; therefore, it is crucial that social attitudes change so the impact of legislative change is not halted.
Sexuality is a contentious issue in society globally. Queer theorist Judith Butler critically highlights the anti-gender discourse rampaging throughout society. The discourse is essentially based upon the opposition to gender ideology and LGBTQ+ rights – a belief often spearheaded by right-wing politics. Butler explores how this movement is incorrectly intrinsically linked to the opposition to equality “for women, lesbian and gay people, trans people, and all those who make their kinship ties in queer ways.”(32) Our society unfortunately still sees any challenge to heteronormativity as an “attack on both the nation and … the ‘natural’ family”.(33) This can be seen by the 112% rise in hate crimes on the basis of sexual orientation in the last 5 years(34) – but note this is only a snapshot of the recorded data; what about all those victims who don’t feel comfortable reporting? It is concerning to note that such views we see in society today mirror those from back in the 1980s. Writing at the time, Kath Weston noted the existence of “common practices that have effectively denied lesbians and gay men from access to kinship”.(35) Unfortunately, we see this ideology against same-sex parents still prevalent today with the restricted access to IVF. The barriers to same-sex parenthood, and the discrepancies in the process of IVF are evidence of the legacy of homophobia that the state, in more recent years, has tried to eradicate through legislation such as the Equality Act 2010.
Even within the healthcare profession, discrimination is still rife. Although the Equality Act 2010 prohibits direct discrimination based on sexual orientation, this does not stop the existence of microaggressions – “subtle derogatory behaviours”(36) – from staff towards same-sex couples. The DIVA survey reported that 7% of same-sex couples experienced some form of discrimination when accessing reproductive or adoption services.(37) An example of such discrimination and microaggressions is noted in the story of Becky and Nancy, a same-sex female couple who went through three pregnancy losses in their IVF journey. Prior to Nancy giving birth to their son, Becky experienced a miscarriage which resulted in hospitalisation. During this time, Nancy was “referred to as a ‘friend’, which completely denied the grief she was experiencing”.(38) It is situations like these in which healthcare professionals create an uncomfortable atmosphere in what can be an extremely traumatic time for any parents, by their own ignorance of a situation. There is clearly still a problem of homophobia towards same-sex female couples accessing IVF, even if not in a direct sense. The consequence of these social attitudes and microaggressions “can lead to distrust and disengagement from the healthcare system”.(39) Subsequently, same-sex female couples are less likely to access IVF due to these social barriers.(40)
This suggests that all this perceived progression in the form of legislation, such as the Equality Act 2010, is simply illusory if society is stuck in this old mindset. We need to address this social issue to effectively increase accessibility.
Immediate action can be taken with the implementation of regular training for healthcare professionals to recognise and address these microaggressions that same-sex female couples are facing when trying to access IVF. Such an approach has been noted by academics: “LGBTQ+ healthcare microaggressions are pervasive and will likely require nuanced training to address them.”(41) Therefore, training should be integrated as part of compulsory professional development programmes for healthcare professionals, with consequences for those who refuse to partake or do not meet the standards. This stricter approach will encourage healthcare professionals to be more aware of their comments and, in turn, reduce microaggressions to make women feel more comfortable to access treatment. This will hopefully have an ‘inside-out’ impact on social views on homosexual families, as the public will see acceptance from healthcare staff, and therefore will alter their view on the issue and begin to change the stigma.
This report has highlighted the financial, geographical and social barriers same-sex female couples encounter when accessing IVF. These barriers leave women feeling helpless, much like the broken ladder analogy. We must therefore repair the ladder, starting with these recommendations: reform of the NHS funding criteria, introduce a payment plan system, impose national standards for funding criteria, utilise technology, and implement mandatory LGBTQ+ training programmes for healthcare professionals. Everyone deserves the opportunity to be a parent; we need to stop making it so difficult for same-sex female couples.
* Kent Law School, LLB with Honours Graduate, 2025. Email ellaking122@gmail.com
(1) NHS, ‘IVF’, https://www.nhs.uk/conditions/ivf/ (last accessed 22 September 2025).
(2) NHS, ‘Intrauterine insemination (IUI)’, https://www.nhs.uk/conditions/intrauterine-insemination-iui/ (last accessed 22 September 2025).
(3) Patrick Steptoe and Robert Edwards, ‘Birth After the Reimplantation of a Human Embryo’ (1978) 312(8085) The Lancet 366.
(4) Pasquale Patrizio, David F Albertini, Norbert Gleicher and Arthur Caplan, ‘The Changing World of IVF: The Pros and Cons of New Business Models Offering Assisted Reproductive Technologies’ (2022) 39 Journal of Assisted Reproduction and Genetics 305-313.
(5) ibid.
(6) Bart Fauser, ‘Towards the Global Coverage of a Unified Registry of IVF Outcomes’ (2019) 38
Reproductive Biomedicine Online 133-137.
(7) Patrizio et al. (n4) 306.
(8) Kate Davison, Katherine Hubbard, Sarah Marks, Hel Spandler and Rebecca Wynter, ‘An Inclusive History of LGBTQ+ Aversion Therapy: Past Harms and Future Address in a UK Context’ (2024) 29 Review of General Psychology 33-48. Aversion therapy in the context of homosexuality refers to a form of behavioural conditioning by which the ‘unwanted’ behaviour of someone's sexuality was paired with discomfort. The aim was to psychologically alter the individual's sexual attraction towards those of the same sex and promote heterosexuality.
(9) Equality Act 2010, section 4
(10) Department of Health and Social Care, ‘IVF Law Change to Benefit Couples with Fertility Issues’, GOV.UK (25 October 2023), https://www.gov.uk/government/news/ivf-law-change-to-benefit-couples-with-fertility-issues (last accessed 22 September 2025).
(11) KANTAR, DIVA, Stonewall, 'The DIVA Survey – LGBT+ Women and Non-Binary People's Insight 2021', Lesbian Visibility Week (April 2021) 18, https://www.lesbianvisibilityweek.com/_files/ugd/6818aa_5ceb7dbf5e8d4d18b128f815ed475fe5.pdf (last accessed 22 September 2025).
(12) NHS (n1).
(13) Rachel Moss, ‘There’s A “Gay Tax” On NHS Fertility Treatment. This Is The Impact’, HuffPost UK Life (15 June 2021), https://www.huffingtonpost.co.uk/entry/gay-tax-same-sex-couples_uk_60b8b0cbe4b02df1ad87f5c5 (last accessed 22 September 2025).
(14) NHS, ‘Find your local integrated care board (ICB)’, https://www.nhs.uk/nhs-services/find-your-local-integrated-care-board/ (last accessed 22 September 2025).
(15) Kent and Medway Integrated Care Board, 'Schedule of Policy Statements for Assisted Reproductive Technologies (ART) for Kent and Medway Integrated Care Board' (June 2024) 9, https://www.kentandmedway.icb.nhs.uk/application/files/7417/1655/8382/Kent_and_Medway_ART_policy_document_June_2024.pdf (last accessed 22 September 2025).
(16) ibid, 9.
(17) ibid.
(18) ibid.
(19) Ibid.
(20) fair4all finance, ‘Nearly half of UK adults now living in financially vulnerable circumstances’ (16 July 2024), https://fair4allfinance.org.uk/nearly-half-of-uk-adults-now-living-in-financially-vulnerable-circumstances/ (last accessed 22 September 2025).
(21) Sabrina Johnson, ‘Influencers Sue NHS After Paying £8,000 on Dream for IVF Baby’, Metro (9 November 2021), https://metro.co.uk/2021/11/09/lesbian-couple-wegan-take-nhs-to-court-over-ivf-discrimination-15562807/ (last accessed 22 September 2025).
(22) Human Fertilisation and Embryology Authority, ‘Family Formations in Fertility Treatment 2022’, (November 2024) section 6, https://www.hfea.gov.uk/about-us/publications/research-and-data/family-formations-in-fertility-treatment-2022/#section-6 (last accessed 22 September 2025).
(23) Human Fertilisation and Embryology Authority, ‘State of the Fertility Sector 2022/23’
(12 September 2023), section 3 https://www.hfea.gov.uk/about-us/publications/research-and-data/state-of-the-fertility-sector-2022-2023/#:~:text=table%20of%20contents-,3.,licensed%20to%20provide%20storage%20only (last accessed 22 September 2025).
(24) Kent and Medway Integrated Care Board (n15) 10.
(25) Olivia Marshall, ‘BPAS Fertility Investigation: NHS-funded Fertility Care for Female Same-sex Couples’, https://www.bpas.org/media/hlldidvj/bpas-fertility-investigation-nhs-funded-fertility-care-for-female-same-sex-couples.pdf (last accessed 22 September 2025).
(26) Chloe Harcombe and Fiona Lamdin,‘Bristol same-sex couple call for fairer access to fertility treatment’ BBC News (16 October 2023), https://www.bbc.co.uk/news/uk-england-bristol-67120914 (last accessed 22 September 2025).
(27) ibid.
(28) Secretary of State for Health and Social Care, Women's Health Strategy for England (CP 736, 2022) chapter 12.
(29) ibid.
(30) Prishita Maheshwari-Aplin, ‘Access to IVF is Still a Postcode Lottery’, Stonewall (18 April 2023),
https://www.stonewall.org.uk/news/access-ivf-still-postcode-lottery#:~:text=Accessing%20IVF%20is%20still%20a,same%2Dsex%20couples%20in%20England (last accessed 22 September 2025).
(31) ibid.
(32) Judith Butler, Who's Afraid of Gender? (Penguin Books UK, 2025) 56.
(33) ibid 51,52.
(34) Stonewall, ‘New Data: Rise in Hate Crime Against LGBTQ+ People Continues, Stonewall Slams UK Gov ‘Inaction’’ (5 October 2023), https://www.stonewall.org.uk/news/new-data-rise-hate-crime-against-lgbtq-people-continues-stonewall-slams-uk-gov-?gad_source=1&gclid=Cj0KCQjwv_m-BhC4ARIsAIqNeBvG_iphf4XMsp-lkdkAocBUnL51dn4YbRt0hjvQjfWB2Jkr0vLKNA0aAhHkEALw_wcB (last accessed 22 September 2025).
(35) Kath Weston, Families We Choose: Lesbians, Gays, Kinship (Columbia University Press, 1997) 21.
(36) Hallie Decker, Ryan Combs, Emily Noonan, Caison Black and Laura Weingartner, ‘LGBTQ+ Microaggressions in Health Care: Piloting an Observation Framework in a Standardized Patient Assessment’ (2024) 71 Journal of Homosexuality 528-544.
(37) The DIVA Survey (n11) 18.
(38) Jessica Bradley, ‘Non‑birthing mums in same‑sex couples discriminated and ignored’, The Lead (6 February 2024), https://thelead.uk/non-birthing-mums-same-sex-couples-discriminated-and-ignored (last accessed 22 September 2025).
(39) Decker et al. (n36).
(40) Stonewall, ‘Sexual Orientation: A Guide for the NHS’, https://www.cht.nhs.uk/fileadmin/site_setup/contentUploads/About_us/Equality/stonewall-guide-for-the-nhs-web.pdf (last accessed 22 September 2025).
(41) Decker et al. (n36).